Overview
Injectable aesthetics is volume restoration — but to restore volume intelligently, you first need a granular understanding of what ageing actually does to the face. This module is not about products. It is about anatomy: how collagen, fat, and bone change across decades, how these changes manifest differently across sexes and ethnic backgrounds, and what the structural principles of volume restoration are before any product decision is made.
The clinical practitioner who understands the ageing face at the anatomical and histological level makes fundamentally different treatment decisions to one who simply learns product protocols. This module establishes that foundation.
Learning Objectives
The Biology of Facial Ageing
Facial ageing is not a single process. It is the concurrent and interacting decline of four anatomical systems: skin, subcutaneous fat, muscle, and bone. Understanding each system, and how they relate to one another, is the prerequisite to any intelligent volume restoration strategy.
1 — Skin: Collagen, Elastin & Hydration
Collagen
The dermis is approximately 70–80% collagen by dry weight, predominantly Type I (structural, tensile strength) and Type III (finer fibres, wound healing). From approximately age 25, collagen synthesis declines at roughly 1% per year. By age 45, a patient may have lost 20% of their peak collagen mass. Post-menopausal women experience an accelerated decline — approximately 30% of dermal collagen is lost in the first five years after menopause, primarily driven by the withdrawal of oestrogen's direct stimulation of fibroblast activity.
Simultaneously, existing collagen undergoes glycation and cross-linking — abnormal molecular bonding that makes fibres stiffer and less organised. UV exposure (Type B/A) dramatically accelerates both degradation and cross-linking via matrix metalloproteinase (MMP) upregulation, explaining why photoageing consistently precedes chronological ageing in visible presentation.
Elastin
Elastin fibres provide the skin's recoil — the ability to return to its resting state after expression or movement. Unlike collagen, elastin fibres are laid down almost entirely in the first two decades of life. The adult dermis does not produce meaningful new elastin. With age and UV exposure, existing elastin undergoes solar elastosis — fragmentation and calcification of fibres, reducing tissue recoil. The visible result is skin that folds rather than springs back, and that loses its ability to adapt to underlying volume changes.
Hyaluronic Acid (HA) & Glycosaminoglycans (GAGs)
Hyaluronic acid is the extracellular matrix's primary hydrophilic molecule, binding up to 1000x its weight in water and providing tissue turgor, plumpness, and volume. GAG production declines with age, reducing tissue hydration and contributing to the flattened, dull appearance associated with intrinsic ageing — separate from wrinkle formation. This hydration component of volume loss is distinct from fat atrophy and is often underappreciated clinically.
Skin quality is a critical variable in assessing volume restoration candidacy. A patient with good skin quality (adequate collagen density, reasonable elasticity) will respond predictably to volume restoration. A patient with markedly poor skin quality — solar elastosis, severe photoageing — has a dermis that cannot adapt to the volume placed beneath it. Restoration in this context often displaces rather than lifts.
2 — Subcutaneous Fat: Compartmental Atrophy & Descent
The subcutaneous fat of the face is not a single layer — it is a collection of discrete, anatomically defined compartments, each with its own blood supply, innervation, and ageing trajectory. These compartments are bounded by retaining ligaments and fibrous septa. Their behaviour is the single most important driver of the visible ageing face.
Fat pads do not simply disappear — they undergo two concurrent processes: atrophy (reduction in volume) and gravitational descent (ptosis). The combination creates the classic signs of facial ageing: hollowing superiorly and accumulation of tissue inferiorly.
3 — Muscle: Hypertrophy, Atrophy & Ptosis
Repeated muscular contraction causes dynamic rhytids that, over time, become static through dermal damage and the loss of recoil described above. With age, some muscles hypertrophy from overuse (masseter in bruxists; platysma as it loses opposing subcutaneous support), while others become less active. The muscular sling that supports facial soft tissue weakens, contributing to gravitational descent of overlying fat compartments.
4 — Bone: Resorption & Structural Support Loss
The facial skeleton provides the foundation on which all soft tissue rests. With age — and particularly dramatically in post-menopausal women — the facial bones resorb. The orbital rim expands (greater volume of space within the orbit), the maxilla retracts (reducing mid-face projection and malar eminence support), and the mandible loses height and width (shortening the lower face and reducing chin projection).
Bone loss directly affects soft tissue position: tissue that was once supported by a fuller maxilla hangs unsupported, exaggerating nasolabial folds and producing a relative descent of the mid-face. Understanding that some patients present with primarily skeletal volume loss — requiring deep periosteal restoration — versus primarily fat pad atrophy — requiring a different plane of approach — is essential to treatment planning.
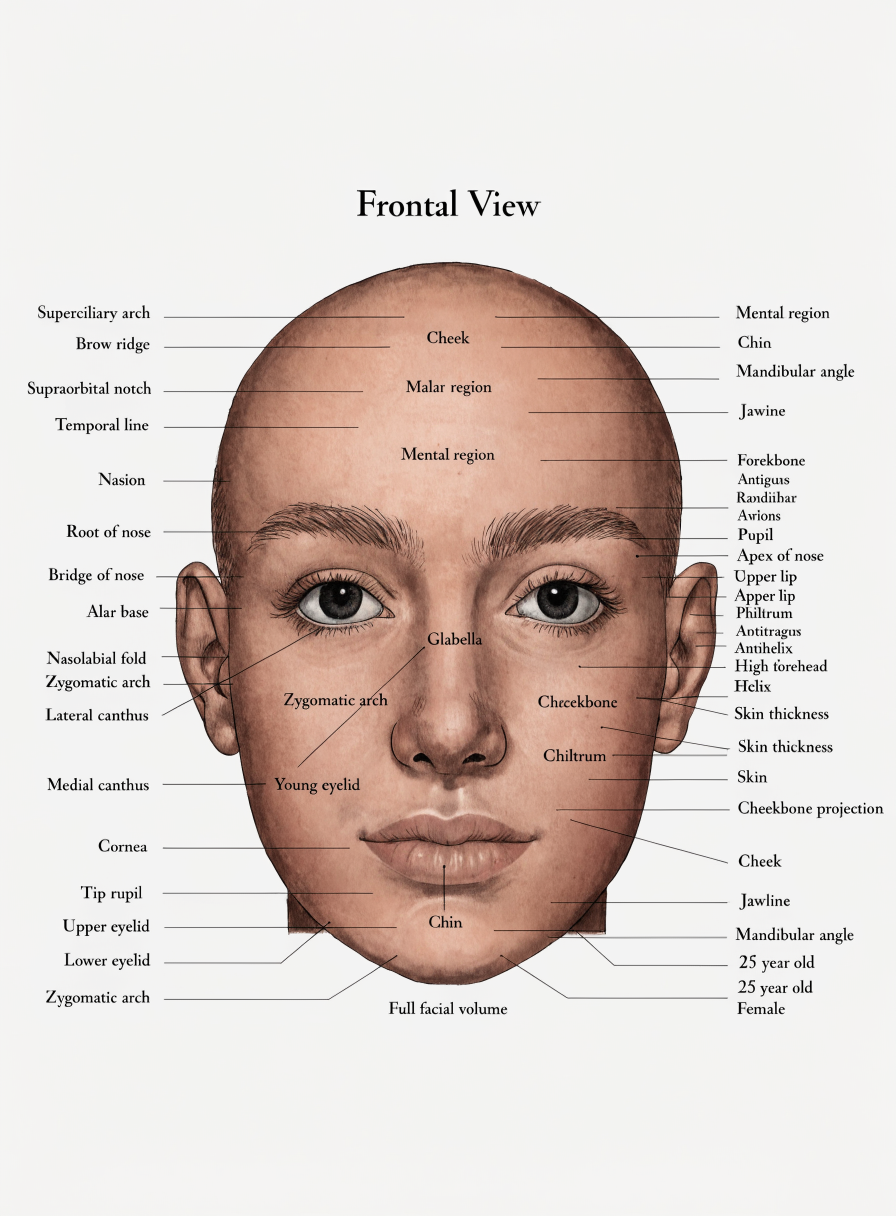
Facial Tissue Layers — Superficial to Deep
The Facial Fat Compartment System
The facial fat pads are the primary drivers of the visible ageing face. Understanding their anatomy, the differences between superficial and deep compartments, and their differential ageing behaviour is essential to planning volume restoration at the correct anatomical level.
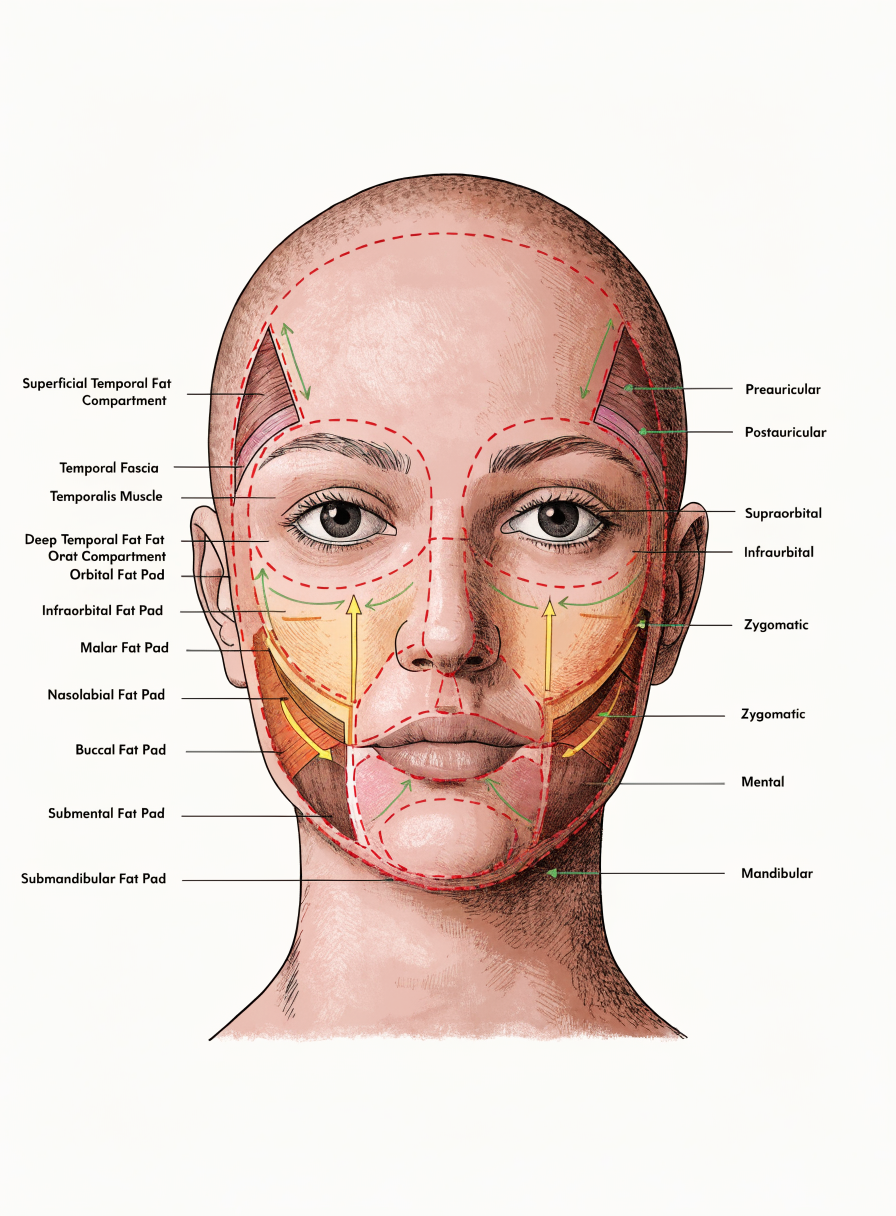
Key Fat Compartments — Clinical Significance
Deep Medial Cheek Fat (DMCF)
The DMCF lies deep to the orbicularis oculi, between the zygomaticus major and levator labii superioris muscles, directly overlying the maxilla. It is one of the earliest deep compartments to atrophy with age, and its volume loss directly subsides the medial cheek and contributes to tear trough and nasolabial fold deepening. Volume restoration at the supraperiosteal plane in this compartment supports the overlying superficial fat and provides structural lift.
SOOF — Suborbicularis Oculi Fat
The SOOF lies beneath the orbicularis oculi in the lower periorbital area. Its atrophy contributes to malar descent and the hollowing associated with the tear trough complex. The SOOF has a superficial and deep component; addressing the appropriate sub-layer is critical to safe periorbital volume restoration.
Nasolabial Fat Compartment
The nasolabial fat sits anterior to the nasolabial fold and descends with age, deepening the fold. Importantly, the fold itself is an anatomical structure defined by a dermal ligament — the nasolabial ligament — not simply a fold of ptotic tissue. Volume restoration medial or deep to the nasolabial compartment supports and elevates it, whereas superficial injection directly into the fold risks visual worsening.
Jowl Fat
The jowl compartment is the primary driver of lower face ageing. It enlarges with age (a combination of true hypertrophy and relative descent as supporting ligaments weaken) and descends inferior to the mandibular border. The appearance of jowling does not necessarily indicate excess fat — it often represents the relative descent of cheek tissue exposing the mandibular margin. Volume restoration in the posterior cheek and above the pre-jowl sulcus can lift the jowl without treating it directly.
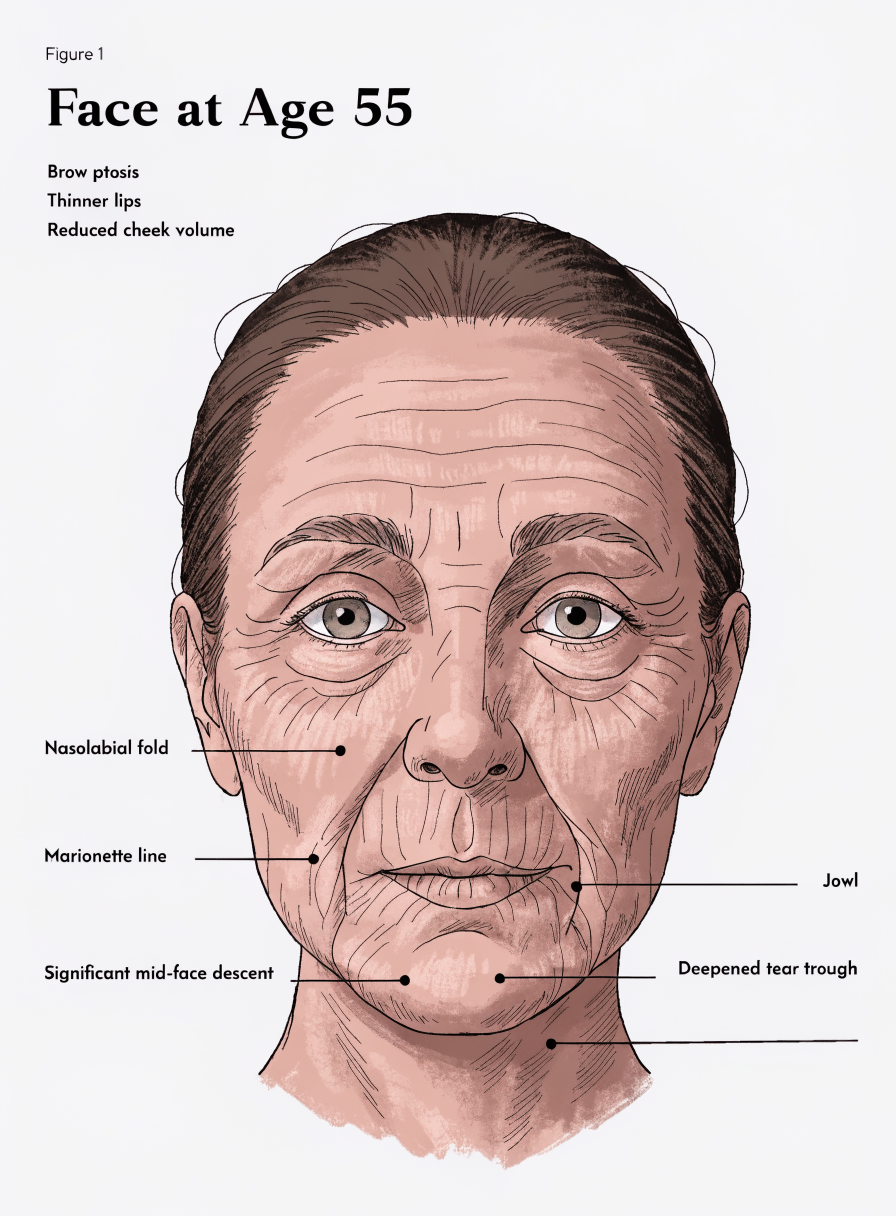
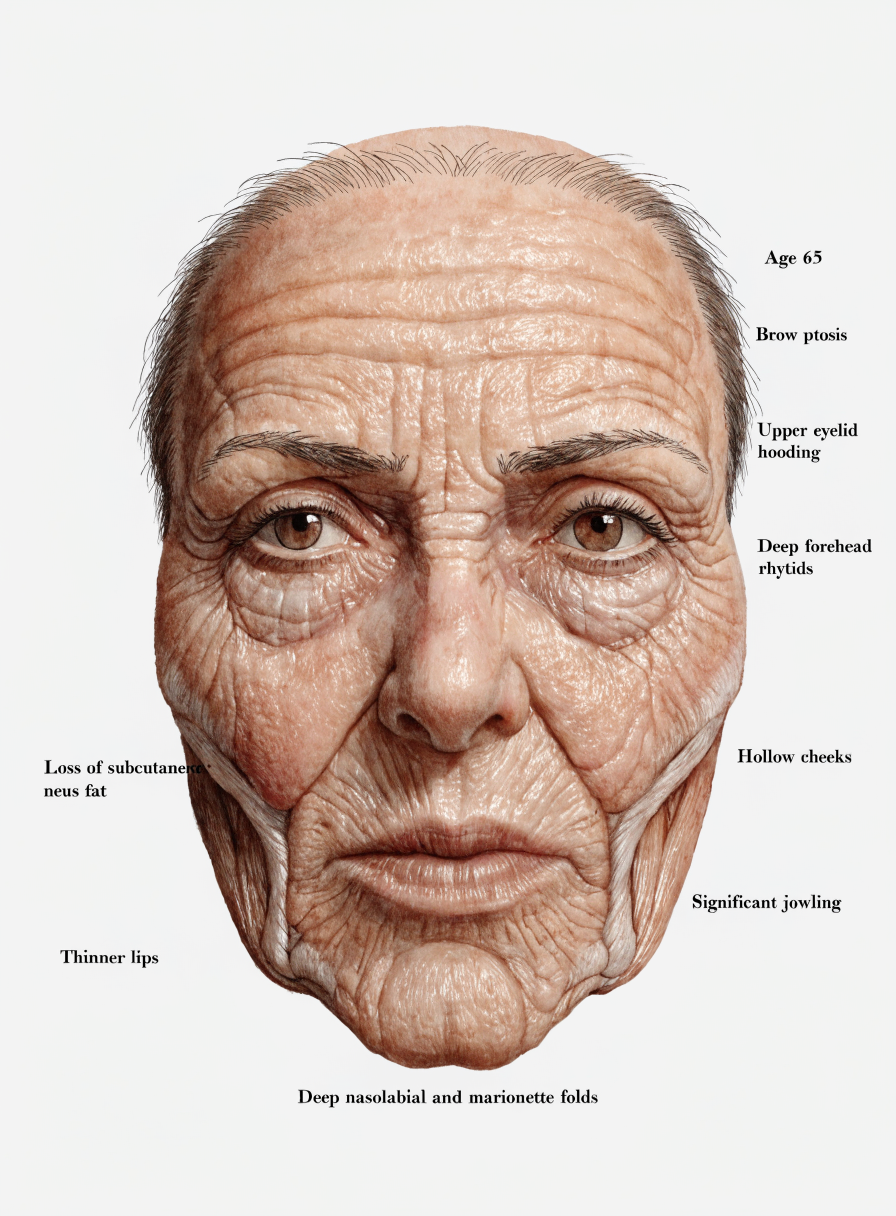
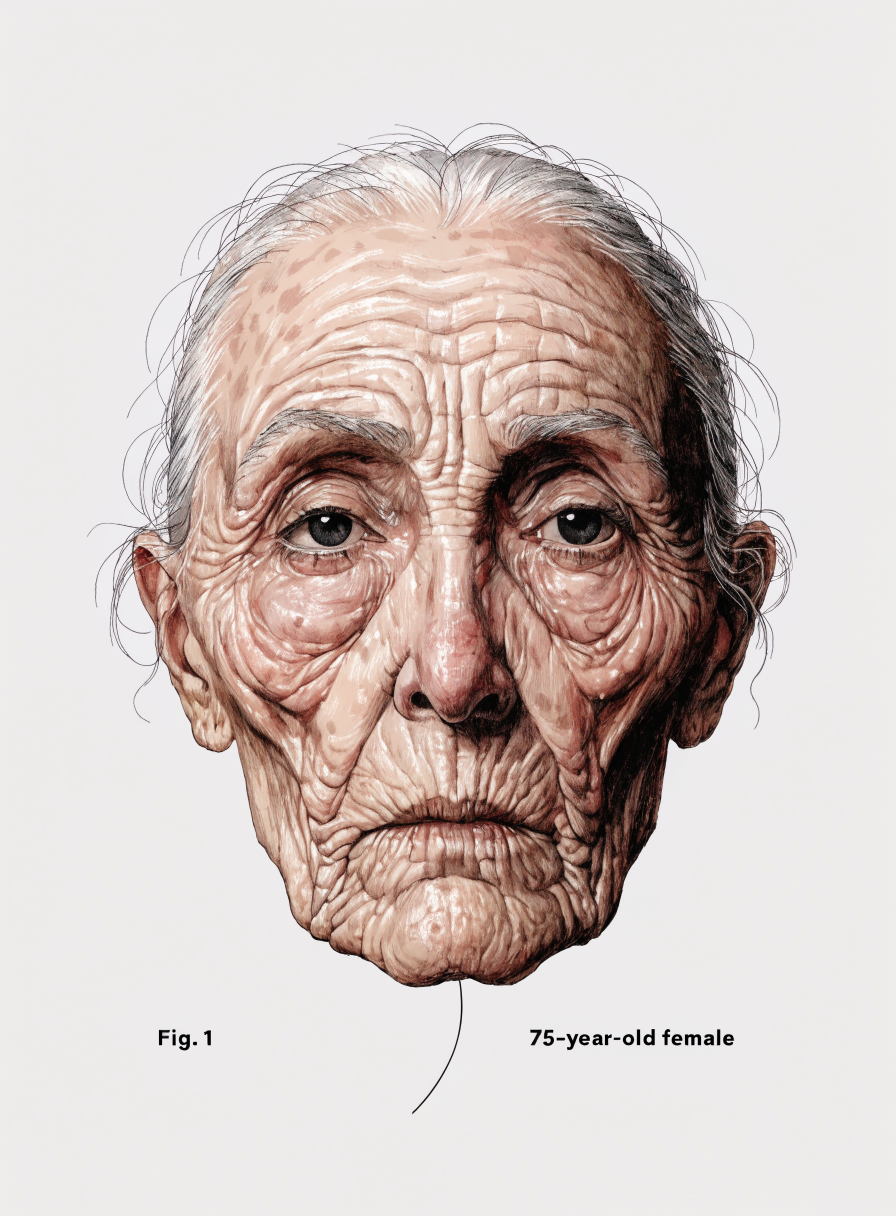
Decade-by-Decade Ageing
Ageing is continuous, but clinically it is useful to conceptualise it in decade-based stages. The following interactive timeline describes characteristic changes across skin, fat, and bone at each decade. Select a decade to explore.
Skin
- Peak collagen density (Type I & III)
- High elastin content — excellent recoil
- Robust HA production; plump, hydrated dermis
- Surface smooth; dynamic lines resolve fully at rest
- Late 20s: first visible signs of UV exposure in high-Fitzpatrick-I patients
Fat & Bone
- All fat compartments full and well-positioned
- Malar eminence strongly supported — "ogee curve" visible
- Facial skeleton at maximum density
- Periorbital area smooth; no hollowing
- Jowl fat contained superior to mandibular border
Predominantly BTX-A for dynamic lines. Volume restoration rarely indicated. Focus: skin quality maintenance (SPF, retinoids). Assessment of early genetic ageing patterns.
Skin
- Collagen declining ~1%/year since mid-20s — 5–10% net loss
- First glabellar and lateral canthal lines becoming semi-static
- Early photoageing visible in lighter Fitzpatrick types
- Skin still rebounds well; elastin largely intact
Fat & Bone
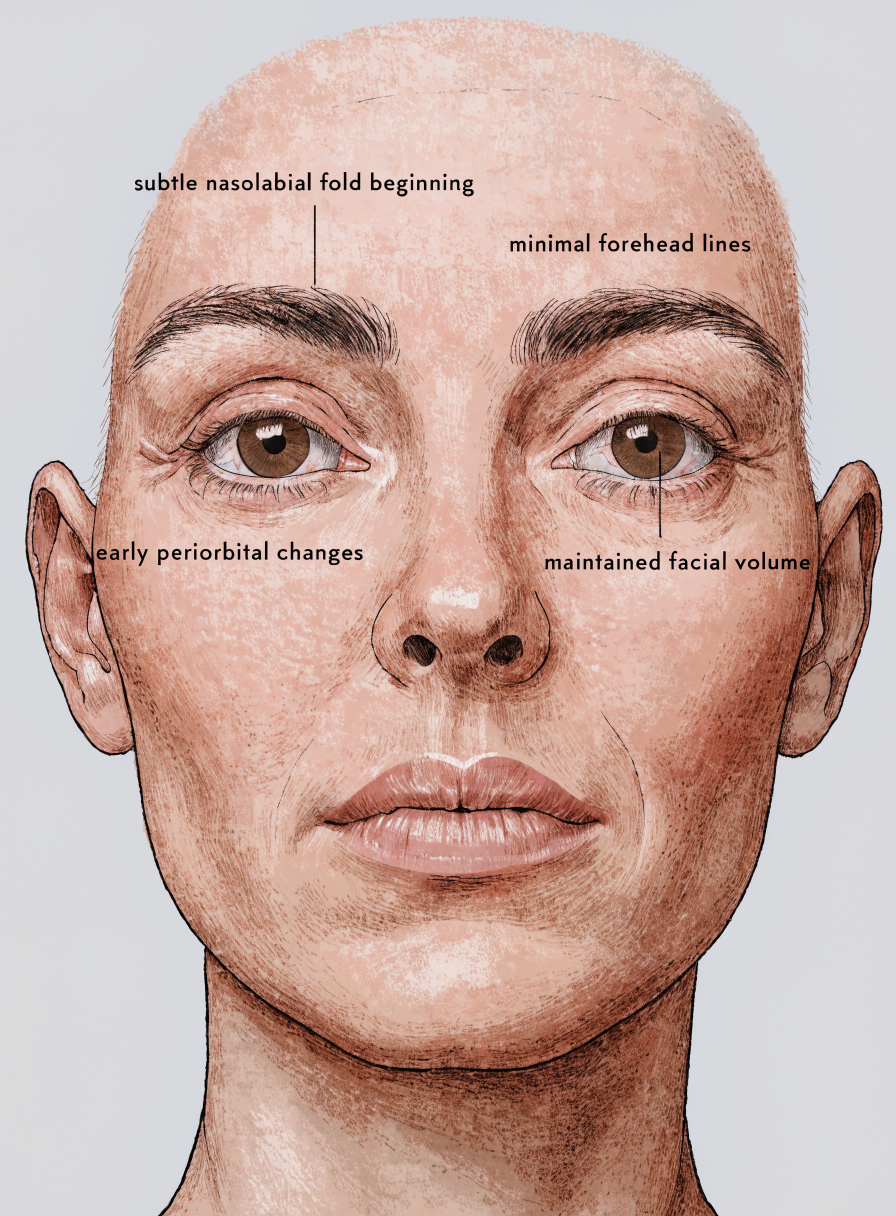
- Early SOOF thinning; periorbital area begins to separate from cheek
- Tear trough becoming perceptible
- Nasolabial fold deepening — NL fat beginning descent
- Malar eminence still prominent but early flattening
- Bony changes minimal; late 30s orbital expansion begins
BTX-A for dynamic lines. Conservative volume restoration: periorbital (tear trough/SOOF), early medial cheek support. Skin quality optimisation. Prevention is still the primary strategy.
Skin
- 15–20% collagen deficit from peak; visible thinning palpable
- Static rhytids now present — glabellar, perioral
- Recoil declining; skin slower to spring back
- Perioral lines (smokers earlier; all patients by mid-40s)
- Significant UV damage visible in Fitzpatrick I–III
Fat & Bone
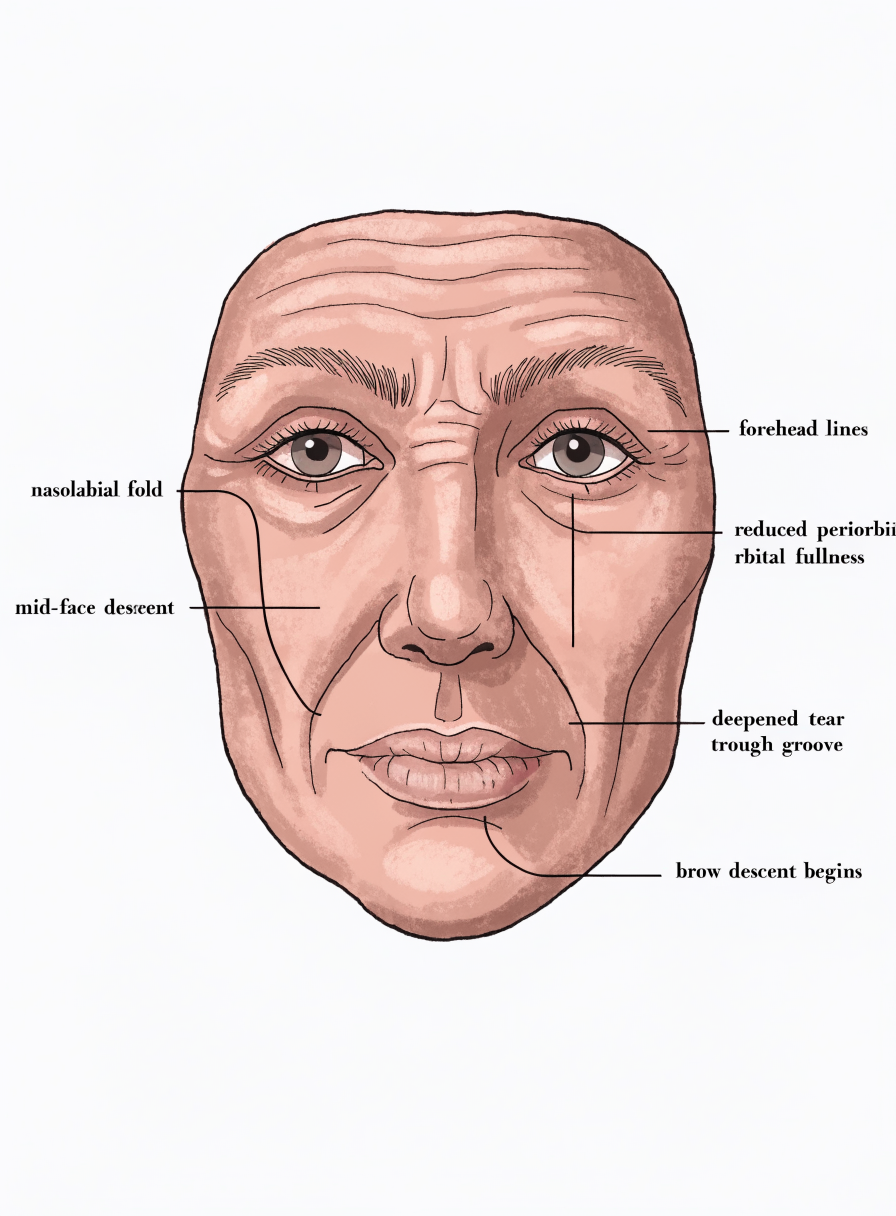
- Malar fat pad descent — loss of ogee curve definition
- DMCF thinning; midface flattening
- NL fold well established — ligamentous component prominent
- Jowl fat beginning to descend below mandibular border
- Orbital expansion (bone) — periorbital hollowing more pronounced
- Maxillary anterior wall begins retracting in women
Volume restoration becomes primary focus. Deep medial cheek (DMCF plane), malar support, periorbital. BTX-A for ongoing dynamic component. Skin quality treatment (resurfacing, biostimulation) as adjunct. Treatment planning requires full facial assessment — isolated area treatment often produces suboptimal results in this decade.
Skin
- Post-menopausal women: 30%+ collagen loss in first 5 years post-menopause
- Skin visibly thinning; perioral rhytids well-established
- Elastin severely degraded; skin drapes rather than recoils
- Significant skin laxity in neck and lower face
- Photoageing effects substantial; pigmentation changes common
Fat & Bone
- Significant deep fat atrophy — DMCF, deep temporal
- Orbital expansion marked — periorbital hollowing prominent
- Maxillary retraction substantial; midface projection lost
- Buccal fat: paradoxical increase relative to atrophied neighbours
- Jowl fat well below mandibular border
- Mandibular border becoming irregular
This decade often requires a structural approach: deep periosteal restoration to address skeletal support deficit before superficial compartment treatment. Patients treated superficially only often show poor longevity and risk tissue displacement. The question is no longer "where are the wrinkles?" but "what structural support is missing?"
Skin
- Marked skin laxity; elastin largely non-functional
- Deep static rhytids across all zones
- Skin can no longer redrape following volume restoration — risk of displacement
- Neck skin laxity significant; platysmal banding visible
- Solar lentigines, pigmentation prominent
Fat & Bone
- Severe deep fat atrophy throughout face
- Orbital expansion marked — eyelid changes prominent
- Marionette lines well-established (ligamentous + gravitational)
- Buccal fat descent contributing to lower face heaviness
- Mandibular resorption — chin projection reduced
- Platysma prominent; supporting structures weakened
Many patients in this decade benefit from a combination approach including surgical assessment. Volume restoration alone cannot address significant skin redundancy. A frank, structured conversation about achievable outcomes — and the role of surgical options — is part of the clinical consultation, not an admission of treatment limitation.
Skin
- Severe skin laxity — redundancy in lower face, neck, décolletage
- Collagen density critically low; skin paper-thin in some areas
- Skin can no longer accommodate volume restoration without displacement
- Extensive photoageing; fragile perioral and periorbital skin
Fat & Bone
- Advanced skeletal resorption throughout facial bones
- Profound fat atrophy — face markedly deflated
- Pre-jowl sulcus prominent; mandibular border irregular
- Temporal hollowing often pronounced
- Neck: platysmal bands prominent; submental volume variable
Many patients in the 70s decade are beyond the threshold for meaningful volume restoration outcomes alone. Skin redundancy exceeds the tissue's capacity to redrape. Surgical consultation — rhytidectomy, blepharoplasty, necklift — is often the primary recommendation. Selective conservative restoration (temporal, tear trough, lip border) can complement surgical outcomes or address specific isolated concerns in appropriate candidates.
Sex-Based & Ethnic Ageing Differences
The ageing trajectory described above represents a generalised framework. In practice, two major variables significantly modify timing, distribution, and visible presentation: the patient's biological sex and their ethnic background. Recognising these differences is not about stereotyping treatment — it is about accurate assessment and appropriate expectation-setting.
Sex-Based Differences
Female Ageing
Female skin is structurally thinner than male skin (approximately 25% thinner dermis at equivalent ages), with lower androgen-driven sebaceous activity. The most clinically significant variable is the relationship with oestrogen: fibroblast activity and collagen synthesis are both directly stimulated by oestrogens. Menopause — typically occurring in the late 40s to mid-50s — causes an abrupt decline in circulating oestrogen and a corresponding acceleration of collagen loss. Studies consistently demonstrate that women lose approximately 30% of dermal collagen in the first five years post-menopause, a rate approximately three times faster than chronological ageing alone.
Female fat distribution features more pronounced orbital and malar compartments in youth, making the loss of periorbital and malar volume particularly visible as ageing progresses. Bone resorption in the orbital rim and maxilla is accelerated in post-menopausal women relative to male peers of the same chronological age.
Male Ageing
Male skin has a thicker dermis, higher collagen density, and higher sebaceous activity — all of which confer some structural protection against early visible ageing. Men typically age more slowly than women in the first four to five decades, but this advantage diminishes and often reverses in later decades as male hormonal changes (gradual decline in androgens) compound with decades of cumulative UV exposure and lifestyle factors.
Male fat distribution tends to be heavier in the jowl and submental areas, with less prominent malar compartments. Ageing in men frequently presents as jowling and neck heaviness before mid-face volume loss becomes the dominant concern. Male patients also present with significant sebaceous hypertrophy — enlarged pores and skin thickening — which must be accounted for in superficial injection planning.
Male patients increasingly represent a growing proportion of aesthetic practice. Male-specific anatomical considerations — denser SMAS, different fat pad distribution, prominent brow ridge, stronger mandibular definition as an aesthetic goal — require modification of standard female-derived assessment frameworks. "Feminising" a male result through overly rounded malar restoration is a common and avoidable error.
Ethnic & Histological Differences
Skin structure varies meaningfully across ethnic backgrounds, with the most clinically relevant differences being dermal thickness, melanocyte density, sebaceous gland activity, and the protective effect of melanin against UV-induced collagen degradation. The Fitzpatrick scale provides a useful clinical starting point, though it captures UV response rather than full structural variation.
| Background | Skin Structure | Ageing Pattern | Clinical Considerations |
|---|---|---|---|
| Northern European Fitzpatrick I–II |
Thinnest dermis; lowest melanin density; most UV-sensitive; fine epidermal texture in youth | Earliest visible photoageing; significant rhytid formation by 40s; prominent skin laxity by 50s. Volume loss often visible before laxity in non-sun-exposed patients | Skin quality often limits volume restoration outcomes — concurrent skin quality treatment important. Low-volume, precise injections due to thin tissue. Bruising tendency higher. |
| Mediterranean / Latin / Middle Eastern Fitzpatrick III–IV |
Intermediate dermis thickness; moderate melanin protection; higher sebaceous activity; more robust fibroblast response | Slower photoageing than Fitzpatrick I–II. Volume loss often becomes dominant concern before skin laxity. Fat compartment changes drive presentation. Malar and NL fold ageing prominent | Good tissue for volume restoration — skin quality typically supports multiple decades of treatment. Risk of post-inflammatory hyperpigmentation (PIH) with needle trauma in darker Fitzpatrick IV patients. |
| East Asian Fitzpatrick III–IV |
Epidermis slightly thicker; flatter facial bone structure (less malar projection, broader midface, flatter nasal dorsum); different fat compartment proportions in youth | Ageing pattern reflects different starting architecture — flatter midface means volume loss presents differently. Periorbital and lower face changes often more prominent than malar changes. Skin quality retained longer | Treatment goals must reflect ethnic aesthetic norms — not a default Caucasian framework. Volume restoration in the malar area requires cultural sensitivity around desired facial shape. Epicanthal considerations for periorbital work. |
| South Asian Fitzpatrick IV–V |
Thicker dermis; higher melanin; sebaceous activity variable; subcutaneous fat distribution varies by region of origin | Slower visible ageing; photoageing less pronounced. Lower face (jowling, submental) often presents before mid-face in many South Asian populations. Skin quality advantage maintained into later decades | PIH risk significant — particularly periorbital. Injections should be precise, with aspiration technique near vessels. Avoid superficial placement where possible to minimise bruising and PIH risk. |
| Sub-Saharan African Fitzpatrick V–VI |
Thickest dermis; highest collagen density; most robust melanin protection; lowest photoageing rate. Dermis can be 2–3x thicker than Fitzpatrick I equivalent | Significant structural advantage — visible ageing typically delayed by 10–15 years relative to Fitzpatrick I–II. When volume loss occurs, often concentrated in temporal and periorbital areas. Skin laxity appears later but can be pronounced once established | Keloid risk must be assessed and discussed. PIH risk highest of all Fitzpatrick groups — needle entry points must be minimised. Treatment planning should account for different baseline structure — goals and volumes vary significantly. Risk of delayed hyperpigmentation at treatment sites. |
Ethnic background informs, but does not determine, treatment planning. Individual variation within any ethnic group is substantial. The role of ethnic awareness in clinical practice is to broaden the assessment framework — to avoid assuming that a patient's ageing presentation will follow the Northern European model, and to set treatment goals that are appropriate to the individual's aesthetic context and priorities.
Volume Restoration: Depth & Plane Principles
This module is not about which product to use. It is about understanding where volume needs to go — and why. The choice of plane determines whether a restoration is structural or superficial, whether it lifts or fills, and whether the result is sustainable or short-lived.
The cardinal principle of facial volume restoration is restore from deep to superficial. Attempting to fill superficial deficit without first establishing structural support at the deep and periosteal levels produces results that are limited in duration, difficult to predict, and potentially displaced by tissue that has no framework to rest against.
Injection Planes — Deep to Superficial
Direct skeletal support. Addresses bony resorption deficit. Primary plane for mandibular border, chin projection, malar/maxillary structural support. High-viscosity, high-G-prime products clinically selected here (not covered in this module). Precise anatomical knowledge required — periosteal plane is adjacent to foramina and neurovascular structures.
Supports superficial fat compartments from below. DMCF, deep temporal, SOOF. Restoration here elevates the overlying superficial compartments via indirect lift — the "scaffolding" effect. Product choice at this plane requires intermediate viscosity and adequate cohesivity to remain anatomically contained.
Direct compartment restoration. Addresses visible deflation in nasolabial, medial cheek, orbital, temporal, jowl areas. Most commonly addressed plane in aesthetic practice. Must follow deep plane restoration where structural deficit exists — cannot compensate for unsupported deep layers.
Dermal hydration, superficial rhytids, fine surface restoration. Appropriate for skin quality restoration (bio-stimulation, skin boosters — covered in separate modules). Requires high tissue integration, low viscosity. Not appropriate for structural volume restoration.
The "Handbag" Clinical Analogy
A useful framework for explaining treatment sequencing to both colleagues and patients: an empty handbag that has lost its structure cannot be restored to its original shape simply by filling it. You first need to restore the frame before the surface material will sit correctly. The same applies to the ageing face — filling superficial deflation without addressing the lost structural frame (deep fat, periosteal support) produces a filled appearance rather than a restored one.
Anatomical Areas and Appropriate Planes
| Area | Primary Cause of Deficit | Restoration Plane | Consideration |
|---|---|---|---|
| Temporal hollow | Deep temporal fat atrophy; temporal muscle wasting; bony resorption | Supraperiosteal; deep to fascia | Frontal branch of CN VII traverses this area — plane selection is a safety consideration |
| Tear trough / orbital hollow | SOOF atrophy; orbicularis thinning; orbital rim expansion | Supraperiosteal / deep SOOF | Highest risk area — thin tissue, prominent vessels, visible lump risk. Assessment of skin thickness is prerequisite |
| Malar / cheek | DMCF atrophy; malar fat descent; skeletal change | Supraperiosteal → deep fat → superficial compartment (layered) | Sequence matters: establish deep support before superficial filling |
| Nasolabial fold | NL fat descent; DMCF loss reducing support; ligamentous tethering | Supraperiosteal medial / deep fat lateral to fold | Direct intranasolabial injection is rarely the correct approach — support from medial and deep planes first |
| Lip / perioral | HA decline; lip border volume loss; perioral rhytids | Submucosal / intradermal / vermilion border | Perioral muscular anatomy — orbicularis oris — must be respected; overcorrection changes function |
| Chin / jawline | Mandibular resorption; pre-jowl sulcus; chin projection loss | Supraperiosteal | Mental foramen — bilateral, located approximately below the second premolar. Periosteal injection anterior and posterior to foramen only |
| Décolletage | Chronic UV exposure; HA loss; collagen degradation; gravitational changes | Intradermal / subdermal (skin quality focus) | Thin skin; high mobility area. Volume restoration not primary approach — skin quality treatment is indicated |
Treatable vs Surgical Threshold
One of the most important clinical judgements a practitioner makes is determining whether a patient's presentation is within the scope of volume restoration treatment or whether surgical referral is the more appropriate primary recommendation. This is not a binary distinction — many patients benefit from both — but the sequencing and framing of that conversation matters.
Volume Restoration Candidate
- Moderate volume loss with adequate skin quality
- Skin elasticity allows re-draping following restoration
- Fat pad atrophy without significant gravitational descent
- Malar descent present but skin redundancy minimal
- Jowling mild-moderate; pre-jowl sulcus addressable
- Patient has realistic expectations of refreshment, not transformation
- Tear trough without significant orbital fat prolapse
- Temporal hollow without significant skin excess
Surgical Consideration
- Significant skin redundancy — tissue cannot redrape
- Jowling severe; mandibular border significantly disrupted
- Significant neck skin laxity with platysmal banding
- Orbital fat prolapse (upper or lower lid) — requires surgical correction
- Ptosis of brow requiring surgical elevation
- Volume restoration would require amounts likely to distort facial proportions
- Patient seeks structural change not achievable with non-surgical means
- Prior volume restoration has failed to achieve meaningful outcome
Attempting to compensate for gravitational soft tissue descent or skin redundancy with increasing volumes of product is one of the most common errors in aesthetic practice. The result is not a lifted face — it is a heavier, wider, rounder face with features that no longer sit in anatomical proportion. The practitioner who can recognise the surgical threshold and refer appropriately is providing a higher level of care than one who treats beyond what non-surgical intervention can achieve.
The Referral Conversation
Recommending surgical consultation is not a failure of non-surgical treatment. It is a demonstration of comprehensive clinical assessment. A useful framework for this conversation with patients:
- Acknowledge what is achievable non-surgically — be specific about what volume restoration can and cannot do for their presentation.
- Explain the mechanism — why their specific concern (e.g. skin redundancy) is structural rather than volumetric.
- Frame surgical as complementary, not opposed — many patients who undergo surgery return for ongoing non-surgical maintenance.
- Provide a pathway — a specific referral to a plastic or reconstructive surgeon you trust, not a vague suggestion.
Learning Check
Select the best answer for each question. Submit when complete.
1. From approximately age 25, dermal collagen declines at roughly what rate per year?
2. The Deep Medial Cheek Fat (DMCF) lies:
3. Post-menopausal women lose approximately what proportion of their dermal collagen in the first five years after menopause?
4. The cardinal principle of facial volume restoration sequencing is:
5. Which of the following is MOST consistent with a patient who is a candidate for surgical referral rather than volume restoration?
Module Feedback
Your input helps improve this content for the practitioner community. Takes 2 minutes.